DIET AND DIETING
Introductory Note:
This book is for you. Written primarily for the overweight, it should prove of equal value to all who have a curiosity or concern about their body, about what makes the machine tick—the human diet. It will show you how to feed that machine for a maximum working efficiency with least breakdown and greatest durability.
The keynote which we shall sound continually is “high-protein.” Young and old, sick and well, underweight, “normal” or obese—a balanced high-protein diet will best provide each of you with the nourishment essential to true health and well-being. And for the overweight, a high-protein reducing diet will help you lose weight painlessly, surely, safely.
Our reducing diet will be painless because it is easy to follow and pleasant to take. No ineffectual calorie counting no flavored yet vomitory mixture or oil to drink—and no starvation! Simply by eating more of high-protein foods (meats that stick-to-the-ribs, “anti-cholesterol” fish, “perfect food” milk and its products), you will set in motion the physiological processes which will reshape your body into what it might have been and can still become.
Our diet is safe because high-protein contains the source materials which your tissues and organs require for constant repair and replacement o£ its minute-by-minute cellular obsolescence. Your body will thus be preserved while you build new muscle structure in place o£ the discarded £at. You do not need to starve your body in order to slim it down.
Finally and of greatest importance, our diet is sure because it attacks the most common cause of obesity, which is overeating or bad eating in response to the false pangs of “chemical hunger.” If high-protein is to be the keynote of this book, then its recurrent theme will be chemical hunger: the gnawing symptoms produced by your blood sugar chemistry.
High-protein kills chemical hunger through regulating your blood sugar levels—we shall see how later. The destruction of this pseudo-appetite will let you diet without having to call upon superhuman control and 24 hour vigilance. It thereby ensures the success o£ your dietary program.
A few decades back it was a political rallying cry that one-third of the nation went hungry. Today, recent polls tell us, one in three persons is contemplating reducing, while about one in five has already made the attempt and backslid. It has also been estimated that about one adult in four is overweight, that is, at least twenty million women and ten million men. You are not alone.
In our fortunate land, for the first time in the history of man, almost all of us can satisfy not only hunger but our craving for the richest and most luxurious foods. The average American today can afford obesity and even heart disease.
A recent Christmas issue of Life featured on its cover page, in place of the woman or man of the hour, an equally glamorous plum pudding flambé, with recipe on an inside page, together with a dozen other luscious and fat-gathering holiday concoctions. On every side, through all the propaganda media, our senses are dazzled by a multi-million dollar processing industry, coaxing our appetite with a vast array of boxes, cans and bottles packaged by Madison Avenue, all begging, “Eat me!” “Drink me!” And it would certainly be nice if we could glut ourselves without fear of consequences.
We are living in a veritable wonderland. Alice in her wonderland, you may remember, partook of the “Drink me” bottle and grew so gargantuan she could no longer see her own feet. Luckily, she was able to dwarf herself down instantly by eating of a bit of cake. If only we had that recipe! It is being sought after as eagerly as explorers once looked for the Fountain of Youth.
Later we shall analyze the various magic formulas, gimmicks and fad diets to learn why they fail. Recently, the 900 calorie merchants have claimed to furnish a brand new full diet containing all the essential food values of protein, carbohydrates and fats, plus vitamins and minerals. But they already had a precursor several years ago in McCall’s miracle diet, a six-ounce goblet of “golden eggnog” drunk seven times a day. When Vogue countered with its own twenty-five day “New cottage cheese diet,” a battle of the women’s mags started. The New York Times Magazine was then moved to comment wryly on the “Great American Dieting Neurosis.”
Women continue to flock to slenderizing salons and people spend millions on do-it-yourself home reducing gadgets. Men and women do a yearly vacation penance at milk farms, health resorts and spas, where they are starved, steam-cabinet, “masseured” and electrically vibrated for a net loss of perhaps five pounds a week, much of it water, at a cost reaching a hundred dollars per pound. They then return home emaciated, but flushed with a hard-won victory, only to recover their fat almost as rapidly and often with a dividend.
The solution seems to point to calorie counting and millions of Americans are doing it. If a calorie surplus produces fat, they reason, then reverse the process. Create a calorie deficit by cutting down sharply on the in¬take of food and you slim out. Yet this doesn’t seem to work very well and we shall see why in a later chapter. Put briefly here, it is less the total quantity of food we eat than the kind, the nature of the calories consumed, that is significant. And this knowledge of food values must be put to work in a long range program.
Overweight is mainly the product of two factors in our lives. As we grow older, our food requirements change. At the same time, we tend to grow more inactive. At the age of twenty-five we already need less and different food than that of the growing period. The decrease in calorie need has been estimated to equal about seven percent for each decade of life. This means that if your body required 3500 food calories at thirty, you may need only 3000 at forty, and at fifty only 2600.
Inevitably, half of the men in their thirties are already ten percent overweight (above an “ideal” weight.) For while the normal appetite decreases, we go on consuming as much and even more, if we include as we must high-calorie alcohol, than in our most exuberant youth. Thus, at thirty, a man’s first bulge appears, at thirty-five a waistline, at forty the paunch.
Even with moderate indulgence we gain weight because we exercise less and less in later years. Older people have always been more sedentary. Before the advent of steam heating, however, their bodies burned many calories daily to keep themselves warm and to maintain a normal temperature of 98.6. Today, our automated industry and farming, gadgeted housekeeping, our motor driven, push-button, television-viewing society has greatly reduced the daily expenditure of energy. The unused surplus of food taken in is converted into fat and stored in tissue throughout our aging bodies.
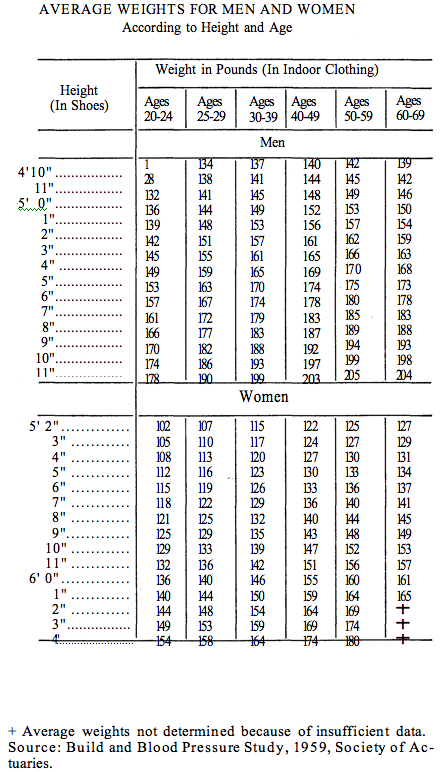
Are you merely plump and appearance-conscious, heavy with little fat, only slightly overweight, or decidedly obese? There is a simple rule-of-thumb by which you can judge. Start with a base of five feet equaling a hundred pounds. Then add five pounds for each inch of your height above five feet for a medium frame, going up ten percent for the large and down ten percent for the small frame. Notice there is no age factor in “ideal” weight since, theoretically, all weight increase should have stopped with your body growth.
Then check the result against the weight table in Chart I of “average” weights, in relation to height and frame, derived from insurance statistics. You may congratulate yourself only if you are at least 10% below the American average—this would be your “ideal,” “desirable” or “best” weight. Actuarial experts tell us there is a proved correlation between “best” weight and our health and life prospects.
While obesity itself has been called a disease, it is in fact a symptom closely associated with numerous dis¬orders. Thus, fat is never listed on the medical certificate as the killer. People die of diabetes, kidney disease, coronary heart disease, a “stroke,” and so on. But we know that fat persons tend to diabetes, that they often infect their kidneys, and that a heart or hypertension case with obesity has a far greater chance of being stricken and less chance for recovery.
You may be overweight without, as yet, showing any grave symptoms. But are you mentally as well as physically vigorous, or sluggish, and do you tire easily? Obesity is also commonly linked with disorders of metabolism, such as gout, and with the minor ailments of indigestion, constipation, muscle pains, etc. It is, in addition, uncomfortable in warm climates or in hot weather and, finally, it is ungainly and sometimes grotesque. There are few nastier epithets than “fat slob.” If the chart shows you as overweight (exceeding even the “average” overweight), you should feel strongly impelled to reduce.
Is all overweight obesity? Your above-average weight may be due less to fat than to a large frame with heavy musculature. Such a person does fine in normal health, but when disease strikes you are none the less more vulnerable. Reduce down to the norm and, if possible, below it. For optimum health prospects we should all approach our “best” weight.
Certainly, an above-average overweight of ten pounds or more is a clear danger signal. If you doubt that you are obese, study your body. There will be puffs of fat in your cheeks; your flesh will billow out and sag. In a man the fat usually collects at the neck and in a ballooning waist, while women gather fat in layers at the breasts and buttocks.
A pinch test may be convincing. Take hold of a flap of skin at the back of your arm or at the side of your lower ribs. You are holding pure fat between your fingers. A quarter of an inch of skin thickness is normal. The excess above this should persuade you that you have let yourself become obese.
Undeniably, the most common cause of fat is overeating, that is, eating more food than your body metabolism can burn. Fat people often hide their secret shame over their condition and its cause by a surface jollity and by alibis which they themselves come finally to believe.
A favorite self-delusion is, “I can’t do anything about it. It’s my glands.” Glandular malfunctioning can be quickly ruled out by your physician. He may order a BMR (to check on the metabolic rate) or, better yet, a PBI (protein-bound iodine blood test), and perhaps also a skull x-ray of the sella turcica, the bony covering of the pituitary gland to see if it is enlarged.
Only two to five percent of obese persons are “glandular.” These can be treated by injections and pills to control the pituitary or thyroid. The normally fat person must look elsewhere for cause and cure.
There is a more common obesity due to faulty metabolism (the rate at which food is burned). Patients say, with a great deal of truth: “Everything I eat turns to fat.” Such people do pose a problem for there is much about metabolism we do not yet understand. If the imbalance cannot be corrected, they must learn to live in terms of their handicap. They are probably eating too much or badly or both.
Others blame their heredity. “It runs in my family,” patients have said. “My parents, my children, we are all this way.” But the hereditary factor in overweight is slight. Frame is inherited, not a tendency to fat. The supposed family characteristic is merely the result of faulty eating habits transmitted by emulation which must now be unlearned.
One sometimes hears frank confession: “I just can’t resist food . . .” “I must have a snack between meals . . . before bedtime … I keep nibbling all day, etc.” “Whenever I feel tense, I eat, mostly sweets. . . .”
Overeating at its various levels may be simple self-indulgence or a defense against outside pressures and inner tensions. And always there is an element of compulsion.
We shall return in Chapter II to these psychological obstacles to weight reduction. Here one can only repeat what every doctor says when faced with compulsive behavior: You must learn restraint, self-discipline! “Appetite grows by what it feeds on.” “Assume a virtue . . .” said Hamlet to his mother. “Refrain tonight and that shall lend a kind of easiness to the next abstinence; the next more easy.”
Yes, all it takes is will power, the very power you have shown yourself lacking in. This advice, known as “boot¬strap psychology,” must always sound a little hollow. Nevertheless, only you can lift yourself up out of your predicament. You will develop the necessary determination when you recognize its value for your health and well-being. Few persons knowingly eat themselves into the grave.
There is an apocryphal story of a physician who shocked severely obese patients into maximum cooperation. He laid before them a life-size photograph of a rat suffering from bulimia. The little creature had been tormented by experimenters, as life harries all of us, into finding an ever-present solace in food through incessant eating. The photo shows him tottering on his tiny legs, his body swollen to the point of collapse. The patient is presumably seized with such disgust that he will never gorge himself again. (By the way, an underfed rat ap¬pears to live longer than a fully fed one, and this may hold true also for humans.)
In most of us, however, a vision of the “body beautiful” should be more compelling than the sight of a bloated rat. What is your mental image of yourself, the real you?
Men tend to see themselves mostly a shade taller than they are, more slender and muscular, really not far re¬moved from the youth of college or senior high school days.
A woman’s self-image is more dependent on social position (slenderness is said to be a female suburban status symbol) and on the latest modes, whether from Paris or the Sears catalogue. She will go seeking a “new self’ in the beauty salon and on shopping sprees, when it is in fact being shaped by her way of life and in her kitchen and dining room.
If you hold before yourself an idealized self-portrait of a healthy body instead of a taunting flesh, it may help fortify your resistance to the insidious vice of even a mild gluttony.
We return to the one person in five who has exercised restraint and then retrograded. A woman patient had over the years gone through a variety of highly touted reducing regimes. Five feet two, she had let herself fatten now to one hundred fifty pounds, an unhealthy condition.
Yet she had periodically succeeded in losing weight on these starvation diets. As an invariable result, her skin would sag into overlapping folds where the flesh (and muscular tissue) had been. Her face and hands, starved of necessary proteins, would wrinkle. She was nervous at work and irritable at home, by her own confession, unlivable-with. And so each time back to the old feeding trough. By now, her health was also suffering from the repeated fluctuations in weight which can be very destructive.
Anybody can reduce by consuming only one thousand calories a day, even when they subsist on ice cream. But at what cost?
Drastic reducing on a “crash” program must bring equally drastic results. For your body will crave all the more the essential food which it has been unjustly denied. The result is a compensatory gorging and a return to former eating patterns, with increasing obesity. Losing weight is not meaningful unless the weight loss is later maintained by a program of intelligent feeding. Don’t look for short cuts, the nine or thirty-day diet. Develop the psychological readiness for the long, the life-long haul.
By all means, eat smaller portions. But remember that a weight loss of over two pounds a week is not desirable. A too stringent curb on necessary food forces the body to consume valuable bone and tissue structure and lowers your resistance to disease.
It is remarkable that, with all the amount and variety of foodstuffs available in our country, a recent study revealed that only twelve percent of a cross-section of the population escaped deficiency in one or more vital food factors. Starvation in the midst of plenty. And, no doubt, many of the undernourished were among the fat and overweight, a double retribution.
What dietary program shall we advocate once we have explained the role that nutrition plays in the human body? By a limitation of certain types of food and a substitution of others, we will help you reduce down to a satisfactory and permanent balance between calorie in¬take and the expenditure of energy. The American tend¬ency to eat softer, sweeter and fatter must be corrected. Only a high-protein diet accomplishes these ends.
No medication is needed. The right foods are in them¬selves curative. When an obese patient comes to me, I map out a diet which may vary with the degree of obesity, the daily expenditure of energy at work, how much he or she can safely lose and how rapidly. No less important is a program of physical exercise suitable to the age, capabilities and daily routine.
Walking is fine, long and vigorous walks of two to five miles a day. Golfing is excellent, if the lost calories are not then replaced in locker room drinking. Tennis, swim¬ming and horseback riding are superlative for the younger obese with strong hearts. Meanwhile, in your daily activity move zestfully, intensely. Indolence and passivity are as conducive to fat as overeating is.
Recently, when a high-protein diet was urged upon an obese patient, Mrs. A., she protested: “But I am on high-protein!” And her smile said, “That’s old hat.”
We checked. She did have an egg each day for break¬fast, about 4 pound of meat or fish for dinner and occasionally some for lunch—and that was it. (No milk or cheese, to which she claimed to be allergic.) The remaining high-protein was supposed to be supplied by vegetable proteins and “enriched” cereals and bread.
Her maximum protein intake per day tallied up to less than 50 grams, just half of what she should be eating. A hundred grams is the daily optimum requirement for the healthy adult, and particularly in weight reduction.
Yes, high-protein is no novelty, any more than some other ideas circulating about, such as peace and brother¬hood. But an idea becomes valuable only to the extent that it is properly understood and applied—and the analogy isn’t altogether far-fetched. When all the nations of the world can offer their peoples more and better protein, we shall be a lot closer to universal peace and amity. We mean better protein than the starvation rice or millet upon which the hundreds of millions eke out their destiny.
We in America who have unlimited Grade A protein foods at our disposal have not yet learned their crucial role in building the body and maintaining its health. Mrs. A., a sedentary housewife, had fattened on “high-protein” that was rather on the sweet and starchy side. She had come to the doctor to ask for an appetite depressant.
“I know I eat too much,” she said. “I can’t understand it but I’m always hungry.” She stuffed herself at the table. Yet, between meals, she felt faint unless she was munching, usually on something sweet. Ashamed of her voracious appetite she nibbled on the sly, away from the family, and had even been awakened from sleep by the urge to pilfer the ice box.
We earlier referred to the psychological stresses that lead to compulsive eating and we devote the following chapter to them. Somehow, to these non-psychiatric eyes, Mrs. A. did not appear psychologically motivated. We knew her as a quite stable person who enjoyed a normal sex life in a fulfilling home environment.
Her hunger pangs, apparently fictitious, seemed very real to her because they were actually experienced. They simulated and exaggerated true hunger and were all the more irresistible. They were symptoms of the “chemical hunger” you read about at the beginning of the chapter. To the doctor they indicated a deficiency of sugar in the blood, in her case we discovered, an extremely low blood sugar level.
If the reader is overweight it is almost certainly due to overeating, though the need may not be as compelling as in Mrs. A. Then, whatever the underlying psychological cause, your false appetite is likewise a manifestation of this chemical hunger. As you read on, you will learn the cause and effect linkage between your food and your blood sugar levels. You will come to understand how a true high-protein diet helped Mrs. A. reduce successfully by killing the hunger pangs which had made her overeat.
We wish we could trumpet out the story of high-protein in tones of command with the selling power of radio and TV. “Reduce by destroying chemical hunger! Banish the midriff bulge! Keep nutrition up and calories down! A fabulous way to a lovely skin—to a new life through . . . I”
This book, however, is dedicated to persuading you with the quieter voice of reason that you can indeed eat your way to better health, appearance and longevity. For the high-protein will safeguard your weight reduction because it strikes at the physiological roots of over¬eating—the low blood sugar of chemical hunger.Written By: Max Konigsberg, M.D. and Louis Golomb, Continue Reading: PSYCHOLOGY OF THE FAT AND THE LEAN
No Comments