Inside Information on Your Intestinal Tract
In order to come to a conclusion or form a judgment with respect to anything in life, it is necessary to have a yardstick of measurement as a basis for comparison. It is for this reason I feel that when I suggest that you attempt an understanding of disordered intestinal function, I also feel obligated to furnish you with a sketch of the fundamental principles of normal intestinal tract function. In this way you can intelligently appraise any deviations from normal or at least recognize them as being departures from normal action.
One of the outstanding characteristics of living tissue is its response to any stimulus that does not kill it. A slight injury to an ameba (one of those large, one-celled, microscopic animals you used to study in the high school biology class), causes it to contract in response to the stimulus which this irritation produces. This principle of reaction holds just as truly in the case of many-celled animals, even such a huge aggregation of living cells as the human body.
It is in this manner that we respond to external irritants and stimuli such as heat and cold, or minute damages such as the prick of a pin or the irritant juice of poison ivy. Since all these things are external to our bodies, we can readily understand how their contact affects us. What most people do not realize is that material inside the food digestion canal is just as much outside of our body as if it were on our skin! It does not really become part of our body until it has been digested by and absorbed from the intestinal tract and thus enters our own blood stream. (Figure 4)
The accompanying diagram shows in greatly simplified manner how food, bacteria, and anything else that is on the inside of your food digestion canal is really outside of you, the person, until these processes described above take place. The truth of this is curiously enough better expressed in a common saying of the laity than by any professional expression I know. Among the boys it is common to hear it said: “I’m going to get on the outside of a nice, big, juicy steak.” A prosaic ambition, no doubt, but a true scientific recognition of the fact that you are outside of your food until it becomes a part of yourself.
Recognizing this makes the understanding of illnesses arising from the food digestion canal quite easy. In other words, an irritant substance placed into this food digestion canal is just as capable of producing symptoms as if it were placed on your skin. Indeed, the various symptoms that result from bowel disease are really due to injuries of various degree which are experienced by the lining of the food digestion canal tube and the nerves in its wall, collectively known as the gastro-intestinal system.
Now we have arrived at the very important understanding that this food digestion canal, this long soft tube, starting at the lips and proceeding down the esophagus, down the gullet to the stomach, through the small intestines and down the large intestine or colon to the exterior is nothing but a channel, or literally a canal, through which material, some of it food, passes through you. Yes indeed, this canal is the busiest traffic channel in the world.
Take it from me, this soft tube does have a hard life of it! Through it are propelled whatever enters the mouth, whether it be solid, liquid or gas. Changed or unchanged, it is pushed along the entire length of the canal, losing here and there whatever substances the digestive juices can, with strange skill, transform into acceptable morsels for those cells lining the canal whose duty it is to absorb what is good and refuse to absorb what is not good.
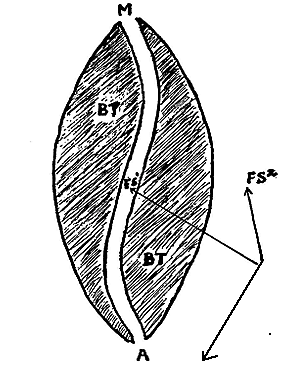 Fig 4. Diagram to show that food inside your intestinal tract is still outside your body until it is digested and absorbed from the food digestion canal, just as truly as if it were completely outside.
Fig 4. Diagram to show that food inside your intestinal tract is still outside your body until it is digested and absorbed from the food digestion canal, just as truly as if it were completely outside.
M — Mouth
A — Anus
MA — Food digestion canal
B — Body tissue
FS — 1 Food substances in canal
FS — 2 Food substances outside canal
The pushing of this mass of material along the tubular canal is brought about by the contraction of the muscles in the walls of the food digestion canal. These, in response to a subconscious stimulus, contract at regular intervals and create the rhythmic ripple of peristalsis, a contractile wave which passes down the stomach along the bowel. The ripple spreads finally down to the colon gathering strength here and there and losing it at other points. The farther down the canal we go from the stomach, the less frequent are these waves though they gain in intensity.
As a matter of information, whereas the ripples come at intervals of every few minutes in the stomach, they occur only every thirty or forty minutes in the beginning of the large intestine. Still further along in the canal, in what is known as the transverse colon, the ripple takes on the nature of a massive push occurring only every five or six hours.
When we get to the pelvic colon, which is almost at the end of the food digestion canal, we find longer periods of quiet but regularly every eighteen or twenty-four hours, a period of active peristalsis, or pushing, occurs and the bowel seeks to expel its contents by giving rise to the desire for a movement. Should this urge be denied through carelessness, neglect, or because one idiotically believes he has something more important to do, then the material stays longer in the pelvic colon or sigmoid than it should. For this insult the guilty party pays dearly in time to come!
Please take a special note of the fact that the material is not stored or retained under normal conditions in the rectum but up above it in the sigmoid. Normally it is held there by a circular muscle until the actual moment of the movement.
Most naturally this very extensive and long continued muscular action, beautifully coordinated as it is under normal circumstances, requires guidance. This guidance is furnished by an internal nervous system whose little twigs are distributed in the walls of the food digestion canal from one end to the other. Please note that these nerves in the lining of the canal are not nerves of sensation. They cannot help you feel pain. They are merely reins on the muscles—reins which impel the muscles toward the contractile state or conversely the state of relaxation.
The first of these, the parasympathetic nerves for which the famous vagus nerve is the chief one, conveys all of the actuating impulses to the muscles and glands distributed along the food digestion canal. They step up action, increase the rhythmic ripple of peristalsis, and relax the controlling sphincter, so that there is no impediment to the onward motion. To balance this action, there are the other nerves known as the sympathetic nerves and these are the ones that manage the contraction of the different segments of the bowel and particularly through the sphincters. They slow down the forward motion.
The action of these two systems of nerves is delicately balanced, so that the functions of the food digestion canal may proceed without disturbance. Their actions supervise, with more or less skill and less, rather than more, judgment by the cerebrum—the home of volition.
I trust I have made matters clear as to the manner in which this food digestion canal functions. Needless to say that with such a complicated mechanism and a delicate one, the possibilities of functional disturbance are great. Except at the extreme ends of the canal and where the bowel is held to the rear abdominal wall, there are no nerves of sensation and this explains why pain all too frequently is only a late symptom of a disease condition.
Departures from normal, however, are readily detected by disturbances of motility of the food digestion canal since these invariably appear early. Thus it is that when an overstimulation of the nerves lining some part of the bowel occurs, a tonic contraction or spasm of the bowel occurs at this point. This disturbs the normal onward passage of the bowel contents coming down from above and in turn causes a distention of the bowel. The distended bowel as it stretches pulls on its attachment to the back of the abdomen and eventually produces pain over certain areas of the abdominal wall and reflexly causes the muscles in certain areas of the abdominal wall to become rigid. Should this irritation in any one spot in the food digestion canal proceed to the point of actual process of disease and extend through the bowel wall to the sensitive peritoneum which covers it, pain becomes intense, if not acute.
Quite short of this, however, the disturbance of the normal motion can bring about a sense of fullness, a pressure distress approaching pain; and very often gurgling, rumbling noises are heard to emanate from the abdomen inhabited by an unhappy food digestion canal. When the ripple of peristalsis strikes this area of impediment to normal function, a back ripple occurs toward the mouth and gives rise to a sensation of nausea. If long continued it can cause vomiting. When the doctor examines you, he will be able to detect the bloating of the intestines and the spasm in certain portions as well as the over-active peristalsis contractions.
You may recall that I stated one set of these internal nerves takes care of the secretions of the glands. Naturally any disturbance of these either prevents the secretion or alters the character of the secretion. Needless to say, any such change, either in the activity or the ability of the digestive glands, renders the process of digestion correspondingly inefficient.
This then, in general, gives you the form and function of the food digestion canal. However, there is a postscript.
As we travel along the canal and reach the middle of the small bowel, we detect the presence of bacteria. This is a normal state of affairs. The body keeps the activity of these bacteria, most of them harmless but some of them harmful, under pretty good control if the motility is normal and the character and quantity of the digestive secretions is normal. They float along with the flotsam and jetsam of intestinal debris. Indeed, by the time they have reached the sigmoid, the bacteria are mostly dead. In conditions of disease, however, they flourish far more than is good for their host.
It is well at this time to point out that it is quite normal for gases to exist in the intestine. They arise partly as a result of air swallowed in the process of eating and drinking or in the process of digestion of food or as a result of bacterial action on certain foods. Whatever their source, they do serve a definite useful function in normal quantities and in normal locality. In that part of the colon between the beginning, the cecum, and the part where it passes the spleen, the intestinal gas helps to propel the intestinal content in much the same way that the air in a pneumatic tube pushes along a mail carrier. Moreover, the gas aids peristaltic action in raising fecal material against gravity.
However, after the colon passes the region of the spleen the gases are of much less value and indeed become a nuisance when abnormal in quantity. Indeed, by distending the sigmoid part of the colon, definite discomfort and actual pain can arise because of the pulling upon the attachment of the colon. This gives rise to a colicky feeling in the left lower part of the abdomen, and to pain that is misreferred to the back and gives rise to the erroneous diagnosis of sacroiliac disease.
In order to understand more clearly the action of bacteria, the following description is offered. In normal quantities, certain types of bacteria are tolerated in the colon. When the lining of the colon, known as the mucous membrane or mucosa, is in good condition, these bacteria are restrained within the colon itself. However, when their numbers become excessive or when the tissue of the colon loses its vitality, the local defenses are overwhelmed and the bacteria will find their way into the liver and eventually to areas of low resistance such as the joints, the roots of teeth, the pelvis of the kidneys and other places. Even more frequently, the chemical toxins which are generated in the colon because of bacterial action are absorbed in quantities greater than the liver can nullify and this leads to many conditions of toxic origin such as lumbago, sciatica, neuritis and arthritis.
The intestinal canal, therefore, has been rightly called the port of entry into the blood stream and has been even more correctly described as the largest and most important potential focus of infection in the body. Many vague ailments, such as allergy, urticaria and chronic headache owe their existence to toxins absorbed from the intestines. Written By: J. F. Montague, M.D., Continue Reading: Departures from Normal
No Comments